Χωρίς τίτλο...
53
Βηματοδότηση χωρίς ηλεκτροκαθετήρες. Τα πρώτα αποτελέσματα από τις κλινικές μελέτες. Ευαγγελία Χριστοφοράτου, * Επιστημονικά Υπεύθυνη Τμήματος Βηματοδότησης Βιοκλινικής Αθηνών * Επιστημονικός Συνεργάτης Α΄ Πανεπιστημιακής Καρδιολογικής Κλινικής ΓΝΑ Ιπποκράτειο Σεμινάρια Ομάδων Εργασίας Ιωάννινα, 13-2-2016
Transcript of Χωρίς τίτλο...

Βηματοδότηση χωρίς ηλεκτροκαθετήρες. Τα πρώτα αποτελέσματα από τις κλινικές μελέτες.
Ευαγγελία Χριστοφοράτου, * Επιστημονικά Υπεύθυνη Τμήματος Βηματοδότησης Βιοκλινικής Αθηνών
* Επιστημονικός Συνεργάτης Α΄ Πανεπιστημιακής Καρδιολογικής Κλινικής ΓΝΑ
Ιπποκράτειο
Σεμινάρια Ομάδων Εργασίας
Ιωάννινα, 13-2-2016

• Technology:
– Highly mature and reliable
– Still includes generator, connectors,
and leads
• Procedure:
– Requires creation of a surgical pocket
– Relies on epicardial or transvenous
leads
• Device/Pocket related challenges
– Discomfort
– Hematomas
– Infection
– Cosmetic concerns
• Leads
– Mechanical failures
– Dislodgement
– Infections
– Extractions
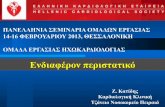
Pacemaker Technology: History and Challenges
Pocket infection Hematoma
Lead dislodgement
Lead fracture
Images: Kabayadondo Maidei Gugu and de Meester Antoine (2011). Early Complications After Pacemaker
Implantations, Cardiac Pacemakers - Biological Aspects, Clinical Applications and Possible Complications, Prof.
Mart Min (Ed.), ISBN: 978-953-307-639-3, InTech, DOI: 10.5772/20091.

First implantable
pacemaker
First microprocessor
based pacemaker
First AutoCapture
pacemaker
First fully wireless
pacemaker
First leadless
pacemaker
Pacemaker Technology: History and Challenges

History of Leadless Pacing: Idea Proposed in 1970
Spickler et al. J Electrocardiol 1970;3:325-331

History of Leadless Pacing: Miniature Pacemaker Tested in 1991
a: Guiding catheter
b: Pusher catheter
c: Miniature pacemaker
d: Steering arm
Vardas et al Eur J Card Pacing Electrophysiol. 1991;1:1-47

Leadless Pacemakers
NanostimTM / SJM MicraTM / MedtronicWiCSTM / EBR
May 2011 December 2012 December 2013

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

What’s Needed for a Leadless Pacemaker?
• Catheter-based delivery system
• High density energy source
• Low power electronics
• Novel communication scheme
• Biocompatible materials
• Dependable fixation design
• Retrievability capability

Nanostim™ Leadless Pacemaker Makes Possible
Leadless Cardiac Pacing
• Energy efficient
– High-capacity CFx battery
– Lower resistance due to lack of lead
– Low-power conductive communication
• Compatible with Merlin™ Patient Care System
• Electrode design is identical to a St. Jude
Medical electrode with same steroid elution
• Designed to prevent dislodgement
– Double fixation: single turn helix (x 2 pull-
strength) plus angled nylon sutures
– Radiographic indicator to ensure proper number
of turns
• Tethered test mode for perioperative
evaluation
• Designed for retrievability
– Catheter-based retrieval system
The Nanostim™ VVIR pacemaker is introduced through the femoral vein
into the right ventricle.

Nanostim: The Device
• Docking feature (A) for delivery, repositioning, and retrieval
• Chemical cell (B)
– Standard cell has 3/4 the capacity of improved CFx
– LCP ASIC uses ¼ the current of standard ASICS
– Result: Same longevity with 3/16 the battery volume
• Compact header (C) with no connector
– Single chip/ASIC senses, paces, and communicates
• Helix (D) provides primary fixation
– Tines add secondary fixation
• Electrode w/ steroid(E) paces, senses & communicates
ED

The Nanostim™ Leadless Pacemaker Delivery System
• Delivery catheter– Soft, flexible, deflectable catheter tip
designed to minimize complications
– Tethered feature
– Integrated protective sleeve
– 18 F
• Handle with four functions:– Steering the deflectable tip
– Docking/undocking
– Rotating the device
– Releasing tether
• 18 F introducer

The Nanostim™ Leadless Pacemaker Retrieval System
• Similar to delivery system– Flexible with deflectable tip
– Integrated protective sleeve
– 18 F
• Either single loop or triple loop
snare
• Handle with three functions:1. Steering the deflectable tip for accurate passage
2. Grabbing and docking the LP
3. Rotating the LP

Nanostim™ Programmer Link
Conductive communication via
surface ECG electrodes
– No bulky antenna
– No added circuit module
– 50x less battery current
than RF systems
– Patented technology

First-in-man LEADLESS study
• Objective: Evaluate the safety and performance of the leadless
pacemaker
• Prospective, non-randomized, multicenter study conducted at 3
European centers
• A total of 33 patients were enrolled– Mean age of 77 years (53-91 years); 67% male
– 67% chronic AF and high degree AV block
– 18% sinus rhythm 2nd /3rd degree AV block with low activity or short lifespan
– 15% infrequent pauses or unexplained syncope
Procedure
• Femoral venousaccess
• LP assessment & programming
Post-Procedure
• 2 View X-ray of pacemaker
• LP assessment & programming
2-week follow-up
• Six-minute walk test
• LP assessment & programming
6-week follow-up
• Six-minute walk test
• LP assessment & programming
3-, 6-, and 12-month follow-ups
• LP assessment & programming
Reddy et al Circulation. 2014;129:1466-1471

LEADLESS Study: Delivery procedure1
• Successful delivery in 32/33 patients (97%)*
• Procedure Times
– Introducer in/out: 28 minute (range 11 – 74 min)
– Catheter in/out: 16 minute (range 3 – 57 min)
• Time from procedure to hospital discharge: Mean 31 hrs (Range 17 – 113)
• Number of times LP was repositioned: Mean 0.5 (Range 0 – 3)
Times LP repositioned Number of patients Percent of patients
0 23 70%
1 4 12%
2 4 12%
3 2 6%
*In one patient, there was cardiac perforation and tamponade which required surgical repair. On
post-operative day 5 after an uncomplicated surgical repair, the patient (who had atrial fibrillation
and was not adequately anticoagulated) had a large right-sided stroke and ultimately expired.
This event was medically adjudicated.
Reddy et al Circulation. 2014;129:1466-1471

LEADLESS Study: LP performance is reliable and
predictable at 12-months post-implant16
Reddy et al Circulation. 2014;129:1466-1471

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I


Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I
up to 720 patients at 70 centres worldwide
140 patients at 23 centres

Micra Transcatheter Pacing Study:
Patient Characteristics
Ritter et al. European Heart Journal (2015) 36, 2510–2519

Micra Transcatheter Pacing Study:
Patient Characteristics
Ritter et al. European Heart Journal (2015) 36, 2510–2519
Implant success rate was 100% (140/140)

• 107 (76.4%) devices were placed at the RV apex
• 33 (24%) were implanted at the anterior septum, midseptum,or
outflow tract
Micra Transcatheter Pacing Study:
X-rays of various device positions in RAO view
Ritter et al. European Heart Journal (2015) 36, 2510–2519

Micra Transcatheter Pacing Study:
Procedure or system-related adverse events from 140 implanted patients
Ritter et al. European Heart Journal (2015) 36, 2510–2519

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Micra Transcatheter Pacing Study:
Patient Characteristics
Ritter et al. European Heart Journal (2015) 36, 2510–2519

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Nanostim: Implantation Procedure
Courtesy of St Jude Medical Inc.

Nanostim (St Jude Medical): The retrieval system
A deflectable catheter with snare (single or triple)
to retrieve the device
Courtesy of St Jude Medical Inc.

Nanostim: Retrieval Procedure
Courtesy of St Jude Medical Inc.

P. Neuzil ESC Congress Barcelona 2014
Implantation Case:
The delivery system places the device to RV apex

P. Neuzil ESC Congress Barcelona 2014
Implantation Case:
Device fixation procedure

P. Neuzil ESC Congress Barcelona 2014
Implantation Case:
Tug test

P. Neuzil ESC Congress Barcelona 2014
Implantation Case:
Contrast Injection

P. Neuzil ESC Congress Barcelona 2014
Implantation in an apically position of IVS

P. Neuzil ESC Congress Barcelona 2014
Inadvertent implantation to LV apex through a PFO

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I

Heart Vessels & Stroke Σάββατο
07/03/2015 Workshop I




![Επαγγελμαικ αποκα `σ Yαση σην επο ] b ης κρσηςstatic.livemedia.gr/hcs2/documents/al11531_us41... · Οειλές ΕΟΠΥΥ ΟΠΑΔ 4 yελεαοι](https://static.fdocument.org/doc/165x107/5e3fff573fa69e36da797d59/-f-yf-f-b-f.jpg)